
This article presents some of the most important need models and how we as therapists can go about helping our clients achieve them. Much of the following his material has been gleaned from Grawe’s work in books Psychological Therapy and Neuropsychotherapy and his work forms the majority of the information offered here.
Epstein (1990) presented four basic needs:
- Need for Orientation, Control, Coherence (consistency principle)
- Need for Joy
- Need for Positive Attachment in Relationships
- Need for Self-Esteem Enhancement and Protection
Panksepp & Biven (2012) present the seven basic emotional systems/instincts:
- Seeking
- Caring
- Play
- Lust
- Fear
- Panic-Grief
- Rage
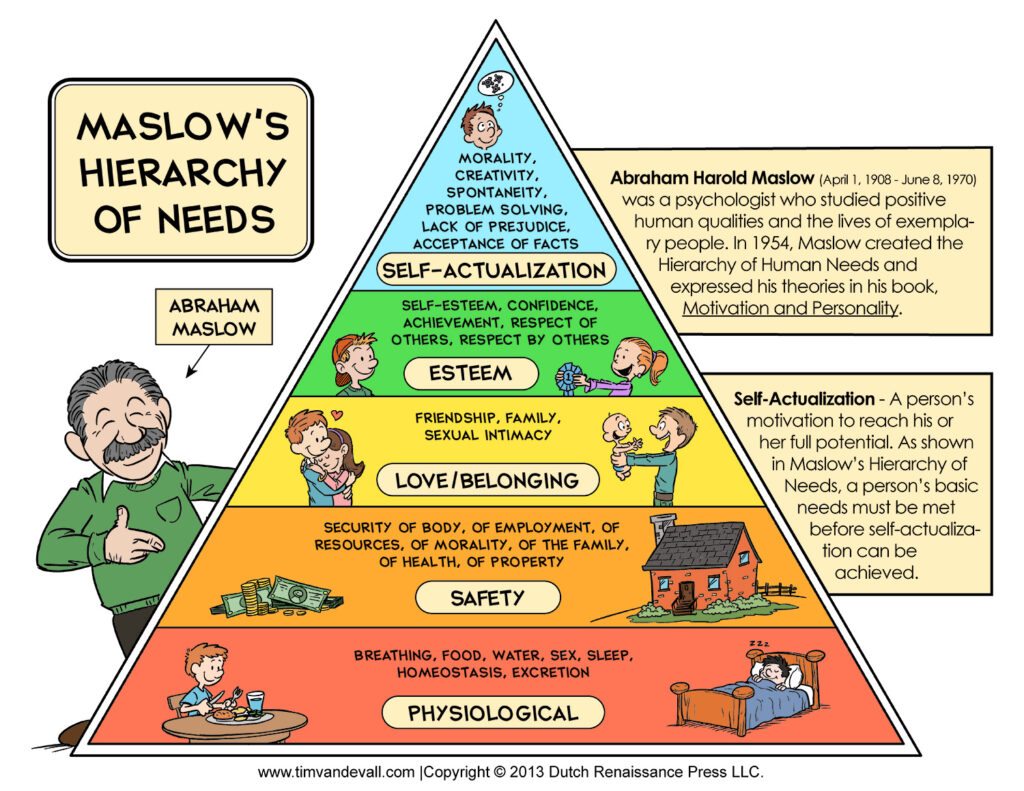
Maslow provides his hierarchy of needs:
Freud provides the pleasure principle as represented in the Id.
How do we help our clients achieve their goals and needs positively?
Motivational Schemas (Grawe, 2007, 2004) work towards achieving your goals. There are two types – avoidance and approach:
- Motivational Approach Schemas are oriented to fulfil our goals/needs.
- Motivational Avoidance Schemas are oriented away from our goals/needs because they have been violated, threatened and disappointed in the past.
Sometimes both types of schemas are triggered at the same time and motivational discordance ensues. This discordance can be triggered by:
- Two approach schemas
- Two avoidance schemas
- An approach and avoidance schema
Discordance between the schemas will manifest in the form of anxiety, anger, disappointment, physiological, hormonal and neural reactions.
Grawe uses the term consistency in working with motivational goals. It is the harmonious compatibility of all mental processes in the achievement of motivational goals and needs. It is good mental functioning.
There are two types of motivational schemas to attain one’s goals – approach schemas and avoidance schemas. Approach schemas orient us to fulfil our goals and needs and they have a clear aim. Avoidance schemas occur when our needs are violated, threatened and disappointed and therefore the client will no longer be motivated to fulfilment of those goals or needs. They actually move away from something they really want or need. There is actually no clear aim at all and if there is an aim it is phrased in a negative way. These clients are established in the violated needs and control by attachment figures early on in our childhood. Sometimes both approach and avoidance schemas are triggered at the same time activating motivational dissonance. Dissonance can also result when two approach schemas are triggered or two avoidance schemas. This dissonance causes anxiety, anger, disappointment, physiological, neural or hormonal reactions. Consistency regulation mechanisms such as defence/coping mechanisms, emotion regulation, incongruence experiences lead to avoidance schemas impairing need fulfilment impairing brain function.
Self-Esteem Needs
The process of moving into more healthy states of mind and away from feelings of inadequacy and inferiority is a process of self-actualisation. One of those goals is the goal of self-esteem, worthiness, adequacy and acceptance of the self. With self-esteem one can better attain the goals of control, pleasure, joy, distress-avoidance, self-image. Self-reflection and communication is required. With this approach one can better address shame, violations of dignity and confronting the effects of negative attachment figures. Where the relationship with the mother has been difficult or even abusive it is actually easier for the client to admit that they were the bad one and the adult was good. It is far easier to manage the disappointment, fear, anger, hopelessness towards the mother when it is internalised into the self and blame unconsciously apportioned within, even when there is a risk of a split occurring within the self in that harmful process. In this process inferiority, inadequacy, guilt, shame, toxicity, low self-esteem and low self-worth manifest. The child then becomes insecure-avoidant, maybe disorganised if we are to apply the attachment theory here. The child cannot criticise the mother because to do so may reap more abuse upon them and maybe worse. Isolation and further neglect may follow. The mother who may be completely unaware of her own behaviours and reactions, lack of availability, sensitivity and responsiveness actually looks for problems in the child and criticises them or another attachment figure, the school or other children. For the child motivational avoidance schemas are born. The attachment figure is not a positive source of love and safety, affection and guidance. The child is lost and exiled.
To increase self-esteem one needs to increase the reality of one’s perceptions, overcoming personal control illusions. Naturally people will often focus on the positive when describing themselves. To increase self-esteem one needs to be more balanced, open to exploring and facing the negative sides of one’s personality. People who are depressed don’t focus on the positive they’re actually more balanced between their own perceptions of themselves and other people’s perceptions of them. It is actually more mentally healthy people who have a skewed perception of themselves. People are naturally optimistic but people with depression don’t share that positivity. Often people with optimistic views are actually self-esteem enhancing themselves. There may be a case for over-optimism but generally it is healthy to have positive expectations. One approach is to be more honest about one’s weaknesses in order for compensatory behaviours and perceptions to be activated and becoming stronger in more aspects of one’s personality.
Freud’s Pleasure Principle
The pleasure principle and Freud’s concept of the Id is not only instinctual but it is also social. Grawe (2007) presents a good example of children under the age of 4 generally do not like beer, wine or coffee but their taste changes due to social factors like group identity and self-esteem. Society may give value to something that we find unpleasant to our personal taste but the social value gradually shifts the taste. In terms of therapy the process is similar because therapy works towards placing value on the thing or things that the client has lost value in. Focusing on the value of something or conditions is important to help the client recalibrate their value system in terms of motivational approach schemas and in doing so decalibrates the motivational avoidance schemas. This process is also reinforced by the two motivational systems – behavioural approach system (BAS) and the behavioural inhibition system (BIS). It is akin to motivational priming. By focusing on positive experiences, preferably internally guided by the client, and if not, guided by the therapist, one can begin the process of allying the client with the more motivational approach schemas, thus activating the left PFC (approach and positive) and deactivating the right PFC (avoidance and negative).
Sometimes the therapist can become a target of the client’s negative perceptions of authority/attachment figures. This transference from the client to the therapist can be an obstacle in the process of therapy so the therapist must be mindful they do not counter-transfer onto a rebellious or challenging client. The therapist needs to see through this and compensate sometimes by exploring the transference with the client but always moving with the core conditions to help the client understand the motivation to help is sincere and authentic. Gradually the client will come round with positive experiences, attachment and control needs met.
Liking or Wanting – Selecting the Goals
What the client wants and likes are two different things because they activate different parts of the brain – they are two different neural processes. Do the goals have motivational salience? The goal that needs to be selected requires dopamine activation for long-term learning to take place. Dopamine energises the approach or avoidance goals. The client is more likely to pursue a goal that has real meaning and is consistent with their motivation. Dopamine is essential. Freud’s concept of the Id is built on the pleasure/joy motivation. Some goals will be inappropriate and primitive in some circumstances and will require inhibition by the superego if we are to use Freud’s model. However, many of the pleasures and joys that we are motivated to satisfy are important and essential goals for ourselves and those around us, such as wanting a warm and safe home, adequate food, secure loving relationships, expression of needs, beliefs and opinions, to control our environment and life activities, self-esteem, respect, etc. All of these things bring satisfaction, joy, happiness and pleasure. Feedback loops in the brain have evolved in order to ensure our purposes are fulfilled. Panic, disgust, pain, anxiety, temperature regulation, blood sugar levels are all developed within us to help us secure positive need fulfilment. They all have neural underpinnings. The need for positive attachment relationships and control are not hedonistic but essential. Food and sex are needs but may become distorted and hedonistic. In the case of addiction this is where the pleasure principle has become distorted, becomes a ‘wanting’ motivation and the expense of other needs and requires recalibration through self-development and awareness and maybe therapy. An avoidance goal like an addiction does displace other more worthy goals and so general well-being suffers and so mental processes require exploration in therapy and consistency restored by applying the consistency theory.
The Consistency Theory (Grawe, 2007)
Inconsistency definition: condition for disorders to form due to simultaneously transpiring mental processes.
Incongruency definition: discrepancy between perceptions and goals.
Inconsistency leads to conflicting mental processes such as approaching a goal/object with a negative thoughts/feelings.
Cognitive dissonance is a form of inconsistency and can be reduced in 4 ways:
- Removal of dissonant cognitions – avoidance, suppression, dissociation
- Addition of new consistent cognitions
- Reducing importance of dissonant cognitions
- Increasing importance of consistent cognitions
Ensuring Consistency
Sometimes clients with enduring resistances to change may react with denial and suppression of facing certain issues. This can be effective for the short-term to manage difficult feelings and situations but persistent denial and suppression can result in non-self-actualisation and adaptation. Self-defeating behaviours, coping and defence mechanisms require making conscious in the therapy in order to move towards redirecting the client to manifesting their goals and needs ensuring consistency.
The ACC is the monitor for pain, sensation, conflict, criticism and competition as well as inconsistency with goal attainment. It mobilises control reactions so therapeutic reflection is required around reactions and accurate assessment of environmental situations to make sure goals are being realised. Depression and anxiety inhibits the ACC and can decrease social engagement so practice in reflection and planning is essential for healthy adaptation to tasks to increase well-being, resolve inconsistencies and mental disorders. Issues like intolerable feelings of abandonment and overwhelm in BPD require exploration and accurate assessment of the environment; worrying requires reflective consideration of usefulness in attaining motivational approach goals in GAD for example; in OCD the controlling, counting and cleaning compulsions require review to assess usefulness in goal attainment and motivational needs around the need for control in life in general. The ACC is essential to maintain efficient operation in making accurate assessments of real situations and the behaviours and cognitions required to meet their needs. In all these disorders control attempts are made in order to maintain consistency but actually have the opposite effect and this needs to be brought to conscious awareness of the client so they can see the need to make choices in alignment with their motivational goals and needs.
Sources of incongruence
Incongruency definition: discrepancy between perceptions and goals.
- current trauma
- loss
- having a bad day
- poor physical/mental health
- attachment styles
- unfavourable attachment behaviour
- problematic consistency-maintenance mechanisms
- dysfunctional cognitions
- motivational conflict
- excessive avoidance
- high symptom severity
- poor well-being
- strong avoidance schemas
- maladaptive interpersonal behaviour
- adverse life circumstances
- lacking resources
- under-developed approach schemas
- lacking awareness of true determinants of behaviour
- unused resources
- ill-being
- psychopathological symptoms
Therapeutic approaches:
- increase utilisation of existing resources
- decrease psychological symptoms like perceptions, avoidance reactions, denial, projection
- reduce depression psychopharmaceutically
- increase positive attachment relationships
- increase control in situations
- increase positive coping strategies – constructive thinking, exposure, perseverance, meditation, relaxation
- decrease avoidance goals
- facilitate approach behaviour
- focus on positive goals
Further Guidelines for Therapy Practice can be found in the Therapist Interventions page.
Bibliography
Epstein, S. (1990) Cognitive Experiential Self-Therapy . In L. . Pervin (Ed)Handbook of Personality: Theory and Research, pp 165-192. New York, Guildford.
Grawe, K. (2007) Neuropsychotherapy. Lawrence Erlbaum Associates Inc. Publishers, USA.
Grawe, K. (2004) Psychological Therapy. Hogref & Huber Publishers, USA.
Panksepp, J. & Biven, L. (2012) The Archaeology of the Mind. W. W. Norton & Company, USA.
© Martin Handy 2022